Prior to the Covid pandemic we performed approximately 300 hip replacements per year.
Hip replacement surgery involves replacing the arthritic hip joint with an artificial joint. This is also known as a prosthetic joint.
The socket in the pelvis, known as the acetabulum is excised and an artificial hemispherical prosthetic socket commonly known as a cup is then inserted into the pelvis.
The ball part of the joint, the head of the femoral bone, is removed. A prosthetic stem is then inserted into the femur (thigh bone) A new ball is then attached to this stem to create the new ball and socket joint.
The new socket and stem are held in place either by a special material attached to the surface of the prosthesis which allows your own bone to grow onto this surface and fix it in place, or else a surgical cement is used to glue them in position. This is very similar to that used in dental surgery to fix metal fillings in place.
The ball, stem and socket can be made from a variety of materials such as metal, plastic and ceramic.
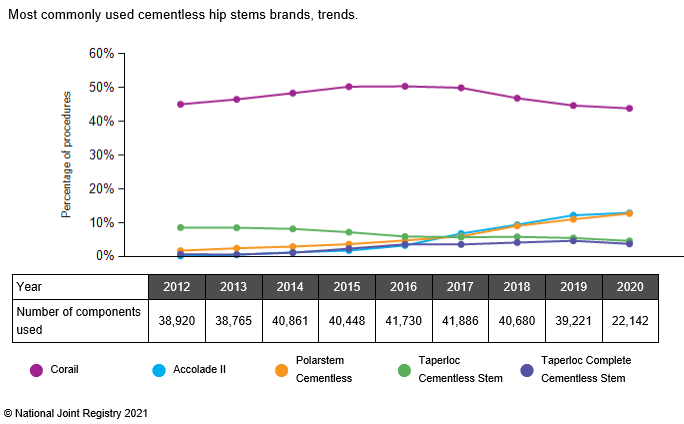
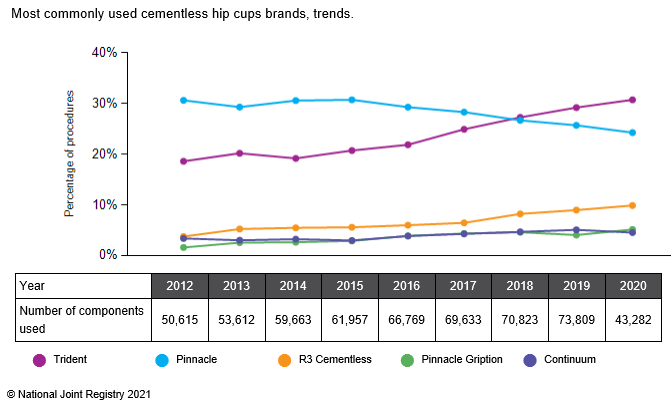
There are numerous hip replacements produced by a variety of manufacturers. In 2011, 142 brands of femoral stem and 119 brands of acetabular cups were available.
We only use prosthetic components with a proven track record. The hip prostheses we use in over 99% of cases are either the Exeter – a stem requiring cement, or the uncemented Accolade II and Corail stems. We have both visited the design centres for these prostheses and learnt the specific surgical techniques for their insertion.
The Exeter stem, designed in Exeter England and currently manufactured by Stryker, is a stem that requires insertion of a grout/cement. It is the most commonly used cemented stem, accounting for 60% of all those used as shown in the graph below.